Sever's Disease and Osgood-Schlatter: A Parent's Guide to Heel and Knee Pain in Active Kids
'Growing pains' deserves a better answer
Your child is 11, plays soccer twice a week, basketball on Saturdays, runs around at school lunch breaks, and one day starts limping after a session. They complain of pain at the back of the heel, or just below the kneecap. You take them to the GP and hear: 'it's growing pains, they'll grow out of it.' That answer isn't wrong — it's just half the story. Sever's disease (calcaneal apophysitis) and Osgood-Schlatter (tibial tuberosity apophysitis) are real, common, treatable conditions in active kids aged roughly 8–15. Knowing what they are and how to manage them keeps your child playing, confident, and avoiding the snowball of deconditioning that comes with months of unstructured rest.
What's actually happening
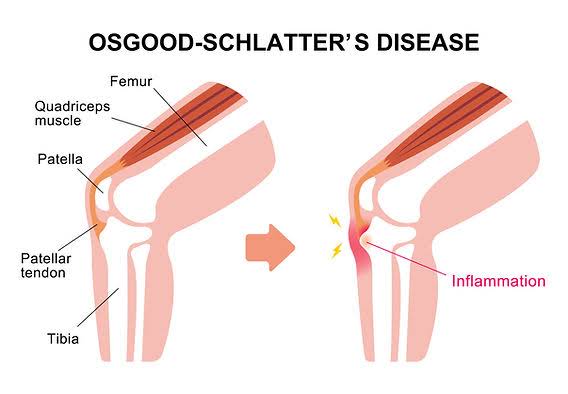
Children's bones contain growth plates at the ends — areas of cartilage where new bone is laid down as they grow. In addition to the long-bone growth plates, there are apophyses: secondary growth plates where major tendons attach. The Achilles tendon attaches at the calcaneal apophysis (heel). The patellar tendon attaches at the tibial tuberosity apophysis (just below the kneecap).
During growth spurts:
- Bones lengthen quickly — within months.
- Muscles and tendons take longer to elongate to match.
- The growth plate at the tendon attachment is under high tensile load.
- Repeated impact and pulling forces (jumping, running, kicking) irritate the apophysis.
- The result is inflammation, pain, and sometimes a visible bony lump (in Osgood-Schlatter).
It's not a tendon injury, it's not a fracture, it's not muscular — it's a growth-plate overload that resolves when the growth plate closes and matures. But the management decisions during that window matter.
Sever's disease — the heel
Typically appears in kids aged 8–13. Pain at the back or underside of the heel, worse after running and jumping, often worse at the start of the next session ('warms up'). Squeezing the sides of the heel reproduces pain. Often bilateral, though one heel may be worse. Common in soccer, AFL, basketball, athletics — anything with running and jumping on hard surfaces.
Osgood-Schlatter — the knee
Typically appears in kids aged 10–15. Pain at the tibial tuberosity (the bump on the front of the shin, just below the kneecap), worse with jumping, kneeling, going up and down stairs. A visible bony lump often develops over months. Common in jumping sports — basketball, volleyball, gymnastics — and kicking sports.
The management framework
Same principles for both, with slight differences in exercise focus:
1. Load modification, not rest
The biggest mistake parents and coaches make is full rest. Six weeks off sport leads to a deconditioned child who returns with the same problem and now also lacks fitness, balance and team connection. Better:
- Reduce the most painful elements — sprint work, repeated jumping.
- Maintain skill, team participation, social connection.
- Replace some on-court time with strength and mobility work.
- Use the 'traffic light' system — green (no pain) = full participation, amber (mild pain settling within 24 hours) = continue with monitoring, red (significant pain or limping) = modify or rest that session.
2. Calf and quadriceps strength
For Sever's: heavy slow calf raises, both straight and bent knee, 3 sets of 10–12, 3x/week. Bodyweight initially, progressing to weighted for older kids.
For Osgood-Schlatter: heavy slow quadriceps work — Spanish squats, leg extensions in pain-free range, single-leg sit-to-stands. Same dose.
Counterintuitive but evidence-supported: loading the tendon attachment helps, in the right dose. The tendon-bone interface adapts to load — it just needs the right starting point and progression.
3. Mobility
Calf, hamstring and quad flexibility lag bone growth. Daily stretching for 30–60 seconds per muscle group helps. Foam rolling can offer short-term relief.
4. Footwear and surface
For Sever's: shock-absorbing shoes, heel cups during sport, avoid running barefoot or in old shoes on hard surfaces. Cross-training on softer surfaces (grass, court) where possible.
For Osgood-Schlatter: a patellar strap can offload the tibial tuberosity during sport for symptom relief.
5. Ice for symptom relief, not as treatment
10–15 minutes of ice after sessions helps with comfort. Doesn't change the underlying condition.
6. Education for the child
Kids handle pain better when they understand it. A 10-year-old who knows their heel hurts because they're growing and their muscles haven't caught up handles the experience better than one who's anxious that something is 'wrong' with their leg.
When to escalate
- Pain that's severe enough to wake the child at night.
- Marked swelling.
- One-sided pain that doesn't fit the typical pattern.
- No improvement after 8 weeks of structured management.
- Loss of function disproportionate to expected.
These warrant medical review and possibly imaging to rule out other conditions (stress fracture, infection, less commonly tumours).
What about other 'growing pains'?
Several other apophysitis conditions exist:
- Sinding-Larsen-Johansson syndrome — pain at the lower pole of the kneecap (the apophysis where the patellar tendon attaches at the kneecap, rather than the tibial tuberosity). Same management as Osgood-Schlatter.
- Iselin's disease — pain at the base of the 5th metatarsal in the foot. Same principles.
- Pelvic apophysitis (anterior superior iliac spine, anterior inferior iliac spine, ischial tuberosity) — common in adolescent footballers and sprinters. Important not to miss; can mimic muscle strain.
The big picture for parents
- This is normal, common, and resolves with growth.
- Your child does not need to stop sport.
- Structured strength work shortens the time and improves the outcome.
- A child who develops a fear of pain or drops out of sport at this age has long-term consequences (fitness, social, motor skill development) far greater than the apophysitis itself.
- Re-flare during the next growth spurt is normal; same plan applies.
Related reading
For older athletes facing patellar tendon issues, our basketball jumper's knee post shares the loading principles. For broader tendon rehab, see 5 common tendon injuries.
Book a paediatric assessment
If your child is dealing with heel or knee pain that's affecting their sport, school sport, or playground confidence — we'd love to help. Sessions are practical, family-friendly, and aimed at keeping kids active. Book an assessment at Evolve Physio & Mastery, Cabramatta. We see junior athletes from across Liverpool, Fairfield, Canley Heights, Bonnyrigg, Bankstown and Southwest Sydney.
References: James et al. 2013 'Sever's disease — a literature review' (J Pediatr Orthop B); Vaishya et al. 2016 'Apophysitis of the tibial tuberosity (Osgood–Schlatter disease): a review' (Cureus); Houghton 2010 review of paediatric overuse injuries.
Frequently Asked Questions
Will my child grow out of it?
Yes — Sever's and Osgood-Schlatter both resolve when the growth plate closes (typically late teens for Osgood-Schlatter, around 14 for Sever's). But 'grow out of it' doesn't mean 'do nothing.' Active management dramatically reduces pain, keeps kids in sport, and prevents secondary problems like deconditioning, motor pattern changes, and dropping out of sport.
Should they stop sport completely?
Almost never. Complete rest is rarely necessary and usually counterproductive — it leads to deconditioning that prolongs the problem. The right answer is load modification: reduce the most painful activities (running, jumping), preserve skill and team participation, add structured strength and mobility work.
Do heel cups or orthotics help with Sever's?
Heel cups and gel inserts offer short-term symptom relief by reducing impact and offloading the Achilles insertion. They're a useful adjunct, not a cure. Calf strength and mobility work do more of the long-term lifting.
When does my child need imaging?
Rarely. Sever's and Osgood-Schlatter are clinical diagnoses based on pattern and palpation. Imaging is reserved for atypical presentations (severe night pain, swelling, unilateral pain with no clear pattern, no response to standard management at 8 weeks) to rule out other conditions.
How long until they feel better?
With good load management and strength work, most kids see noticeable improvement in 4–6 weeks. Full resolution of pain tracks with growth plate maturation, so flares can come and go through growth spurts over 12–18 months.
Is this an injury that will affect them later in life?
Generally no. Sever's leaves no long-term problems. Osgood-Schlatter occasionally leaves a small bony lump at the tibial tuberosity but rarely causes ongoing pain in adulthood. Far more important is keeping the child active and confident in their body through this period.

